

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Approximately 14% to 20% of all intracranial aneurysms originate along middle cerebral artery (MCA) [1]. Among those MCA aneurysms, aneurysms of the M1 segment are second in frequency to bifurcation aneurysms. Aneurysms at proximal M1 segment represent 2% to 12% of all MCA aneurysms [2]. They are composed of lenticulostriate artery or anterior temporal artery saccular aneurysm.
Spontaneous thrombosis of a saccular aneurysm is known to occur, and occurs in about 40% of giant aneurysms. It may be symptomatic secondary to mass effect or stroke. However, spontaneous thrombosis of non-giant (<25 mm) saccular aneurysm is much less identified [3].
We report a case of fully thrombosed non-giant aneurysm which mimics intra-axial tumor with peripheral rim enhancement in magnetic resonance image (MRI). In addition, we reviewed the literatures of thrombosed aneurysm which mimics intracranial tumor.
CASE REPORT
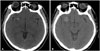
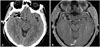
A 54-year-old male patient, with a history of traffic accident a week ago, presented to the hospital with sustained headache after the accident. 7 years ago, he had taken the brain computed tomography (CT), and small mass like lesion was found in right frontal area (Fig. 1). He was lost to follow-up since then. The CT scan taken this time showed enlargement of the mass-like lesion with surrounding edema (Fig. 1). To evaluated the mass, brain MRI was taken. The MRI showed dark signal intensity on T2-weighted images and peripheral high signal intensity on T1-weighted images with peripheral rim enhancement (Fig. 2). Additional studies such as diffusion-weighted MRI, perfusion MRI, magnetic resonance spectroscopy or angiography were not conducted considering poor financial status of the patient. Differential diagnosis included intra-axial tumors such as glioma, metastatic tumor or ganglioglioma.
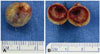
We performed the operation using a right pterional craniotomy under general anesthesia. Navigation-guided transcortical approach was performed, and the mass was exposed (Fig. 3). The lesion was found to be a large thrombosed aneurysm originating from the M1 segment of right middle cerebral artery. We applied one vascular clip at the parent artery and the distal end was coagulated by bipolar coagulator. After cutting the parent artery distal to the vascular clip, thrombosed aneurysm was totally removed (Fig. 3). Pathologic examination confirmed the diagnosis of thrombosed aneurysm. It showed aneurysmal sac with organizing thrombi and atherosclerotic change (Fig. 4). Postoperative images showed total removal of the lesion (Fig. 5). Postoperative angiogram was done to confirm the vascular clip applied to the proximal right middle cerebral artery and to rule out other abnormal vascular lesions (Fig. 6). The patient recovered well and discharged a week later.
DISCUSSION
Intracranial aneurysms are common and affecting approximately 5% of the population [4]. And MCA aneurysms represent approximately one third of intracranial aneurysm [5]. Furthermore, aneurysms of the M1 segment represent 2% to 12% of all MCA aneurysms [2]. Proximal MCA aneurysms can be further divided into superior wall type and inferior wall type [6]. Superior wall type of M1 segment aneurysms arise at the origins of the lenticulostriate arteries and project into the frontal lobe. Inferior wall type aneurysms arise at the origin of the anterior temporal artery or the temporopolar artery and project toward the temporal lobe in an anterolateral projection. This case belongs to the former subtype, superior wall type of M1 segment aneurysm. The thrombosed aneurysm was projecting superiorly into the frontal area. The aneurysm of this case can be classified as a lenticulostriate artery aneurysm. Lenticulostriate artery aneurysms are rare entities, especially rare in patients without underlying comorbidities such as moyamoya disease, mycotic aneurysms, other vasculopathies, or hypertension or drug use in adults [7]. In addition, when they have been reported, they are typically associated with hemorrhage [7].
Giant aneurysms, which are bigger than 2.5 cm in diameter, are unusual, representing 5-13% of all intracranial aneurysm [8]. These giant aneurysms usually present as masses rather than hemorrhages. In addition, spontaneous thrombosis of an intracranial aneurysm is well known usually in giant aneurysms [9]. Black and German [10] demonstrated the relationship of aneurysmal volume and aneurysmal orifice to intraaneurysmal thrombus formation by biophysical and hemodynamic studies. A larger ratio of volume to orifice causes slower flow and longer blood retention time, resulting in intraaneurysmal thrombosis. This is the reason why giant intracranial aneurysms have a high incidence of thrombus formation compared to common size aneurysms. However, in this case, thrombosed aneurysm was 1.9 cm in diameter which is defined as "large" aneurysm rather than "giant" aneurysm. And it was even smaller when it was first detected. In this case, location and size of the mass was not easy to consider thrombosed aneurysm as a differential diagnosis. So, this case shows that surgeons should consider thrombosed "large" aneurysm as a differential diagnosis when the size and location of mass is not typical as other giant aneurysms or other thrombosed aneurysms.
There have been many reports of other intracranial lesions wrongly diagnosed as intracranial neoplasms. For example, tuberculoma, which is tuberculosis of the central nervous system (CNS), has been a lot reported up to now [11]. CNS tuberculomas have the ability to mimic a brain neoplasm and can develop in any region of the CNS. It is the result of hematogenous spread from a primary focus in the lung [12]. In clinical field, it is not so rare to misdiagnosed thrombosed aneurysm as a brain tumor, however, thrombosed aneurysms mimicking intracranial neoplasm have been reported only in 4 cases previously (Table 1) [13,14,15,16]. It might be because it seems not so valuable to report. But, in this case, it seemed valuable to share, because as mentioned above, it was not so big as giant aneurysms and the location of aneurysm was lenticulostriate artery which is rare. Among the other reported cases, the aneurysms of 2 cases [13,16] were included in a category of giant aneurysm and the aneurysms of 3 cases [13,14,16] were located in posterior circulation. Every patient of the reported cases was managed successfully by controlling the parent arteries and totally removing the thrombosed aneurysm, and the outcomes were excellent. There were no efficient imaging tools to differentiate between these thrombosed aneurysms and intracranial neoplasms. Conventional angiography and diffusion restriction MRI were not sufficient for differential diagnosis [13,14,15,16]. In our case, both studies were not done because of poor financial status of the patient. However, as the aneurysm was fully thrombosed, both studies would not be useful for diagnosis in this case. Therefore, when a patient presents with an intracranial lesion lying on the course of major cerebral arteries or even on the course of distal cerebral arteries, it is important to have thrombosed aneurysm in mind as one of the differential diagnosis. Though full studies of MRI and conventional angiography are recommended in suspected cases, the clinician must be aware of the limitations of imaging studies in identifying thrombosed aneurysms. Furthermore, in these cases of thrombosed aneurysm, though it has low possibility of rupture because it is fully thrombosed, the surgeon should control the parent artery completely by clipping or trapping to prevent intraoperative or postoperative arterial bleeding.
In conclusion, we report a rare case of thrombosed large aneurysm mimicking intra-axial brain tumor. Peripheral rim enhancement with surrounding edema in MRI can be easily diagnosed as a brain tumor. However, when the lesion is lying on the course of major or distal cerebral arteries, it is important to have thrombosed aneurysm in mind as one of the differential diagnosis and be prepared when surgically treating such lesions.




 XML Download
XML Download