

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Trigeminal schwannomas (TSs) comprise 0.07-0.36% of all intracranial tumors and are the second most common type of intracranial schwannoma following the vestibular variation, which account for 0.8-8% of intracranial schwannomas [1,2,3,4,5,6]. TSs may arise from the trigeminal nerve root, the gasserian ganglion, or one of the three peripheral branches, contributing to their complicated developmental pattern. Comprehensive knowledge of the anatomical features of TSs is essential in planning surgery to achieve complete tumor resection. In the current report, we present modified classification of TSs that considers not only the location of the tumor, but also its shape and extension into the adjacent compartment. We also discuss our own experience in managing these tumors with different surgical approaches according to their classification.
MATERIALS AND METHODS
Patients
The Asan Medical Center Institutional Review Board granted a waiver to dismiss the requirement for informed consent and approved the chart review (S2014-1069-0001). We retrospectively analyzed 49 patients with TS who were treated surgically by a single neurosurgeon at Asan Medical Center between 1993 and 2013. Patients with type 2 neurofibromatosis and/or those who had undergone previous operations were excluded from this study. Patient demographics, presenting symptoms, neurological examination findings, operative findings, neurological morbidities, complications, and recurrence of tumor were obtained from the medical records.
Radiologic evaluation
Tumor characteristics (size, location, and extent) were evaluated using computed tomography and magnetic resonance imaging (MRI). A preoperative gadolinium-enhanced MRI was obtained in all patients, and the first postoperative MRI was obtained 3 months after surgery. Subsequently, patients were reviewed either annually or biannually with follow-up MRIs.
Classification
Trigeminal schwannomas are classified according to their location of origin and extension into adjacent structures. Type M tumors are confined to the middle fossa, originating from the gasserian ganglion or the peripheral branch at the lateral wall of the cavernous sinus; Type P includes tumors confined to the posterior fossa, originating from the root of the trigeminal nerve; Type MP represents tumors involving equally both middle and posterior fossae; Type E tumors are placed in the extracranial space. E1, E2, and E3 represent involvement of extracranial V1, V2, and V3 branches, respectively; and tumors that belong to type ME are dumbbell-shaped and involve both the middle fossa and extracranial space. Small letters represent the compartment that is adjacent to where the tumor extends; Type Mp tumors are predominantly located in the middle fossa with posterior fossa extension; Type Pm tumors are predominantly located in the posterior fossa with middle fossa extension; and type Me1, Me2, and Me3 are middle fossa tumors involving extracranial V1, V2, and V3 branches, respectively (Fig. 1).
RESULTS
Clinical characteristics
A total of 49 patients (22 males and 27 females) were included in this study. The median age of the patients was 40 years (range, 21-75 years), and the median follow-up duration was 28 months (range, 1-14 years). The most common presenting symptoms were headache (83.7%), ipsilateral facial numbness (67.3%), dizziness (24.5%), facial pain (22.4%), hearing disturbance (18.4%), diplopia (16.3%), gait disturbance (14.3%), hemiparesis (8.2%), incidental finding (6.1%), seizure (4.1%), ptosis (4.1%), and pathologic laughter (2.0%). Duration of symptoms ranged from 2 weeks to 7 years.
Classification and surgical approaches
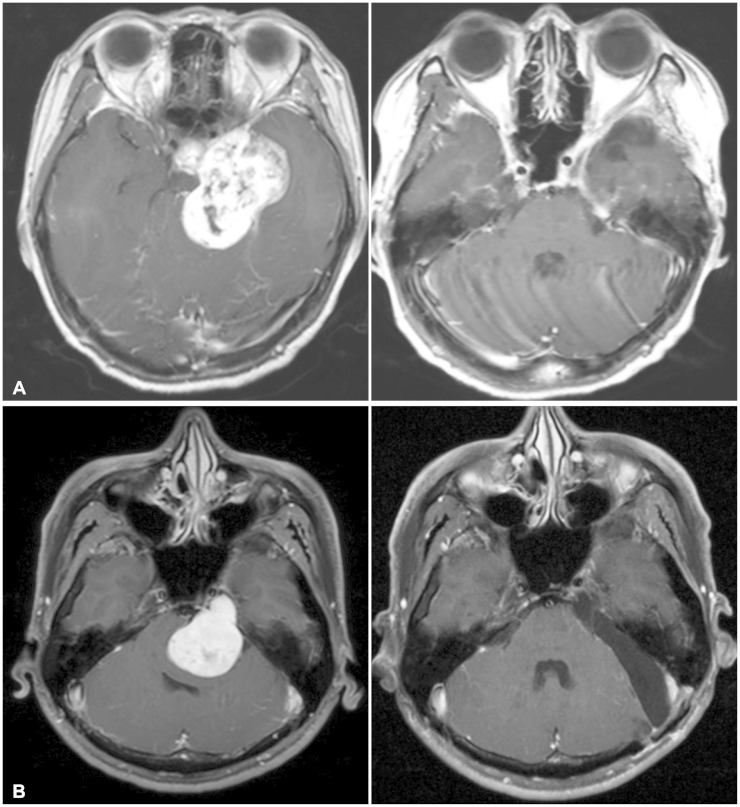
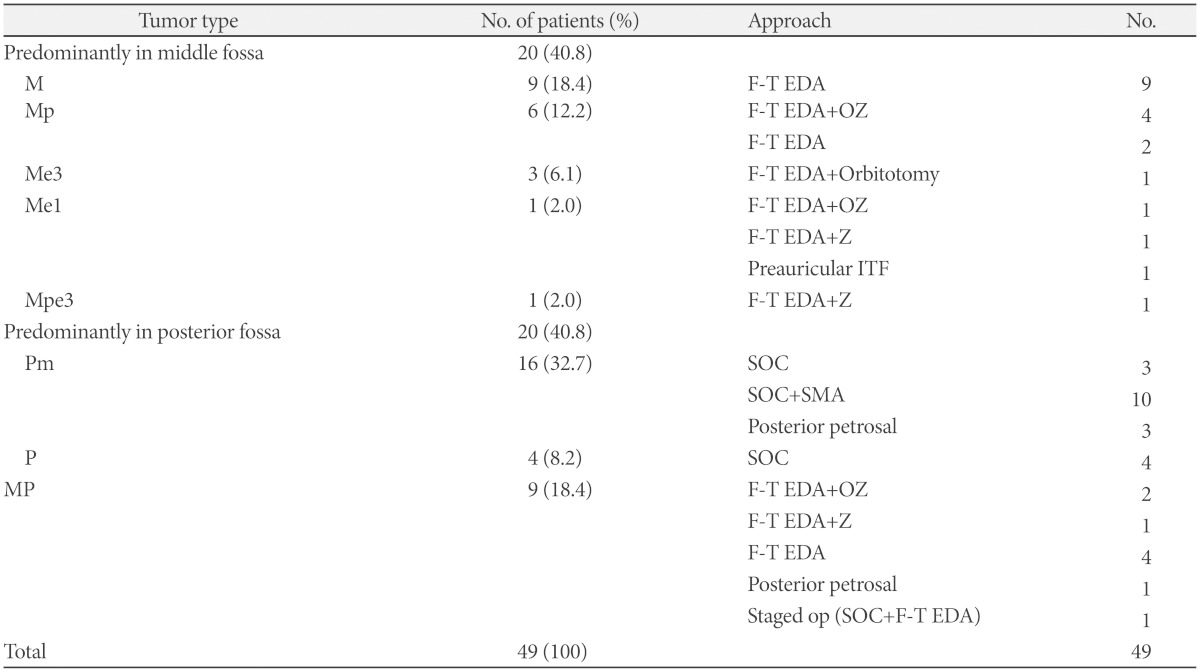
Surgical approaches according to the classification of TS are summarized in Table 1. A frontotemporal craniotomy and extradural approach were applied to most of the tumors that were predominately located in the middle fossa, such as type M, Mp, and Me tumors, as well as type MP tumors (Fig. 2A). An additional orbitotomy, zygomatic osteotomy, or orbitozygomatic osteotomy was performed according to tumor extension. A lateral suboccipital craniotomy with or without a suprameatal approach was performed for most of the type P and Pm tumors (Fig. 2B). The four tumors that involved both middle and posterior fossae (three Pm and one MP) were operated via a posterior petrosal approach. One patient with huge type MP tumor received a two-stage procedure, which comprised of a lateral suboccipital craniotomy and frontotemporal extradural approach.
Surgical outcomes
Gross total resection was achieved in 47 patients (95.9%), and subtotal resection was carried out in two patients (4.1%). One patient with subtotal resection was treated with cyberknife radiosurgery for the residual tumor, and the other patients remained under close observation.
Clinical outcomes
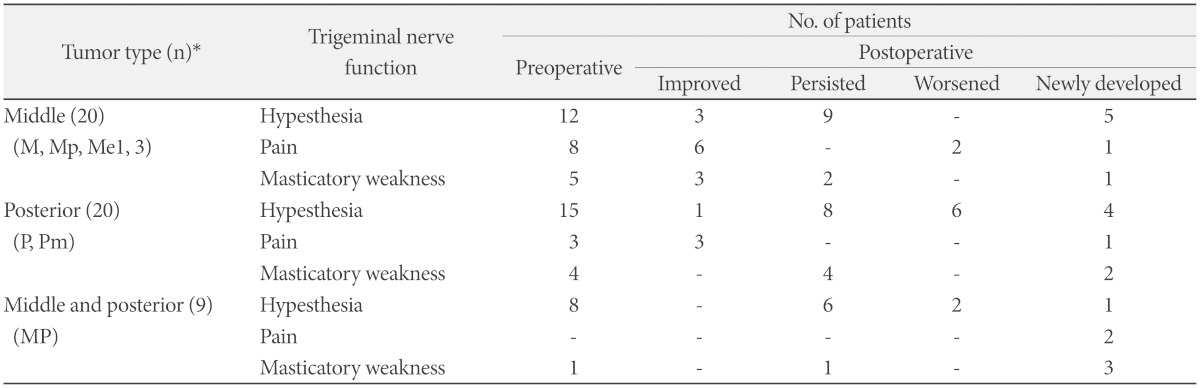
Preoperatively, overall trigeminal dysfunctions were observed in 37 patients (75.5%). Facial hypesthesia was observed in 35 patients (71.4%), facial pain in 11 patients (22.4%), and masseter weakness in 10 patients (20.4%). Postoperatively, trigeminal symptoms were improved or unchanged in 25 cases (51.0%), and these symptoms seemed to be associated with tumor location (Table 2). Facial hypesthesia persisted or worsened after surgery in most of the cases. More specifically, hypesthesia improved in only 25% of the patients with a middle fossa tumor, 6.7% of the patients with a posterior fossa tumor, and no patient with a type MP tumor. Facial pain was more frequently presented in tumors originating from the middle fossa (40.0%) than those from the posterior fossa (15.0%), which tended to be more frequently resolved in the middle fossa tumors (25%) than the posterior fossa tumors (0%) after surgery. Masseter weakness improved in 30% of the patients.
Recurrence
Recurrence occurred in two patients (4.1%) who had received gross total resection at 23 and 42 months. One patient was stable without further disease progression, while the other patient underwent gamma knife radiosurgery.
Surgical complications
The most common postoperative complication was meningitis (5 patients, 10.2%), followed by cerebrospinal fluid (CSF) leakage (3 patients, 6.1%). Of the three patients with CSF leakage, two were treated by lumbar drainage and one patient required surgical treatment. In one case of type M tumor that extended into the cavernous sinus, the ipsilateral internal carotid artery (ICA) was damaged during removal of the tumor. Subsequent ICA trapping and an arterial bypass were performed. The patient suffered from postoperative cranial nerve III and VI palsies during the immediate postoperative period; however, the symptoms were completely resolved 3 months after surgery. There was no mortality in any of the examined cases.
DISCUSSION
Classification
Trigeminal schwannomas most commonly arise from the gasserian ganglion, but may also originate more proximally from the trigeminal root or more distally from one of the three post-ganglionic divisions of the trigeminal nerve; the ophthalmic branch is the site of origin more frequently than either the maxillary or mandibular branches [6]. Largely, there are three classification systems used today to describe TS. The first classification system was proposed by Jefferson [7] in 1955 who categorized TSs into three different types: Type A, which described tumors originating from the gasserian ganglion in the middle cranial fossa; Type B, which comprised of tumors originating from the roots of the trigeminal nerve in the posterior fossa; and finally, Type C, or the so-called "hour-glass" tumors, which occupy both the middle and posterior fossae. Some authors have added a fourth classification, Type D, tumors with extracranial extension [8,9,10]. In 1986, Lesoin et al. [11] classified TSs into three categories: Type I schwannomas, which originate from the roots of the posterior fossa; Type II schwannomas, which originate from the gasserian ganglion; and Type III schwannomas, which originate from the trigeminal branches. Yoshida and Kawase [12] proposed a classification that categorized TSs into six types: Type P, which comprise posterior fossa tumors originating from the root of the trigeminal nerve; Type M, which comprise middle fossa tumors originating from the gasserian ganglion or the peripheral branch at the lateral wall of the cavernous sinus; Type E, which include tumors arising from the extracranial peripheral branches of the trigeminal nerve; and Type MP, ME, and MPE, which indicate a combination of P, M, and E tumors. We modified Kawase's classification to offer information about the locational predominance, shape, and extension of the tumor into the adjacent compartment by representing them with capital (primary location) and lowercase letters (extension).
Clinical features
Trigeminal nerve dysfunction is a presenting complaint in 70-95% of patients with TS, and includes numbness and/or paresthesia in one or more of the three trigeminal branches, facial pain, and atrophy of the masseter muscle [8,12,13,14]. One study reported facial hypesthesia in 11 of 16 patients (68.8%) by the time of diagnosis, while another study reported 13 of 27 patients (48.1%) had facial hypesthesia preoperatively [6,12]. In our study, facial hypesthesia was observed in 76.2% of the patients. The reported incidence of facial pain at presentation varies from 10% to 45% [8,13,14,15], and can be either typical trigeminal neuralgia or atypical facial pain. The facial pain seems to be associated more with tumors originating from the gasserian ganglion than those from the trigeminal nerve roots, although there are controversies [16]. In our case series, facial pain was more frequent in tumors originating from the middle fossa (40.0%) than from the posterior fossa (15.0%). It has also been suggested that constant facial pain is more associated with middle fossa schwannomas, which may be attributed to the relatively fixed position of the gasserian ganglion in the trigeminal impression of the petrous bone, while intermittent facial pain is closely related to posterior fossa schwannomas compressing more mobile trigeminal roots. Weakness of the temporalis and pterygoid muscles was reported in up to 60% of cases in one large series, however, most series have reported an incidence between 25% and 35% [10,13,14,17]. Trigeminal nerve-related symptoms, such as numbness, facial pain, and wasting of the masseter muscle are useful in diagnosis TSs [18]. Although trigeminal nerve dysfunction is a common presentation in TSs, some patients can be asymptomatic. Given that TSs grow slowly with vague initial clinical features, diagnosis of TS is often delayed and most of the tumors are found to be large in size at the time of operation [8,9,18].
Surgical approaches
Many surgical approaches have been described for each type of TS. For type M tumors, Pollack et al. [6] reported two cases where TSs were less than 3-cm in size and could be totally resected via a frontotemporal extradural and intradural approach. Yasui et al. [19] reported two cases of total resection via an orbitozygomatic infratemporal approach. Yoshida and Kawase [12] remarked that the frontotemporal extradural and intradural approach is the most straightforward surgical strategy for type M tumors. On the other hand, Zhang et al. [5] used a frontotemporal craniotomy with or without zygomatic osteotomy, while Fukaya et al. [1] suggested that the optimal surgical approach for type M TS is a subtemporal approach.
For type P tumors, Yasui et al. reported two cases of total resection via transpetrosal transtentorial approach. Yoshida and Kawase [12] used the lateral suboccipital or anterior transpetrosal approach. Zhang et al. [5] used a lateral suboccipital craniotomy. Fukaya et al. [1] suggested that the optimal surgical approach for type P TS is an anterior transpetrosal approach.
For type MP tumors, Yasui et al. [19] used a transpetrosal transtentorial approach or a two-stage operation using a fronto-pterional approach after a lateral suboccipital craniotomy. On the other hand, Fukaya et al. [1] and Yoshida and Kawase [12] performed their operations via an anterior transpetrosal approach. Zhang et al. [5] reported that various conventional and skull base approaches are required for type MP tumors because of their complexity, such as the extradural-transdural-transtrigeminal pore approach via a frontotemporal craniotomy and orbitozygomatic osteotomy, and the temporal base transtentorial approach via a subtemporal craniotomy.
Surgical outcomes
Advances in surgical techniques over the last 50 years have been mirrored by better resection rate with reduced mortality and morbidity. For example, Jefferson [7] described six operative cases that included two deaths and one recurrence in 1955. In 1960, Schisano and Olivecrona [20] reviewed nine surgical cases with a mortality rate of 40%. A study by Konovalov et al. [21] of 111 cases, of which 28 were performed between 1962 and 1977, reported a total resection rate of 68% and a 7% mortality rate. Following the introduction of the microscope, the total resection rate improved to 78% with a mortality rate of 1% between 1978 and 1989. The application of skull base techniques between 1990 and 1994 further improved the total resection rate to 87% with zero mortality. Overall, there has been an improvement in total resection rates from as low as 33%, with conventional approaches, to 84-100% with skull base techniques [8,10,12,13,21,22,23]. This can advance be easily visualized in the total resection rate reported by Yoshida and Kawase [12], which was 33% with conventional approaches and 94% for skull base approaches. Moreover, Sarma et al. [23] reported 26 cases that were all completely resected using skull base techniques. The skull base technique offers more success as it provides a wide exposure of the mass and facilitates more complete resection of the tumor [8,14,21]. In the current series, the total resection rate was 95.2% with no mortalities. The most frequent reasons for residual tumors were that they had infiltrated into the cavernous sinus or that they adhered to the brainstem. It should be noted that, even when complete microscopic resection is thought to have been achieved, small pockets of tissue can still be left in the cavernous sinus, and this is often the most common site of recurrence. In the current study, gross total resection was achieved in 47 patients (95.9%) with no mortality. Of the two cases of subtotal resection, one was a large-sized MP-type tumor, which was firmly adhered to the dura of the posterior fossa, while the other case was a Pm-type tumor where the residual tumor was found in Meckel's cave by MRI after surgery. In the latter case, the residual portion of the tumor was not visible with a microscope, and adjuvant cyberknife radiosurgery was applied 28 months after the initial operation.
Facial pain has been reported to be relieved after surgery in 73% to 100% of cases [8,13,14,15]. However, only 19-44% of patients show an improvement in facial hypesthesia [8,13,14,15]. Furthermore, trigeminal motor dysfunction, which includes wasting of the pterygoid and temporalis muscles, show poor recovery rates [8]. In our series, 81.8% of patients showed an improvement in facial pain, whereas only 11.4% recovered from facial hypesthesia. In terms of masseter weakness, 60% of patients recovered from the symptom, but this result might be attributed to recall bias or limitations of the retrospective study. Meanwhile, tumors that were predominantly located in the middle fossa showed better postoperative trigeminal functional outcomes than of those in the posterior fossa, suggesting that preganglionic nerve injury was more critical in trigeminal dysfunction than postganglionic damage.
Recurrence
The recurrence rate of TSs in older surgical series before 1990 ranged from 0% to 25%, while more recent series have reported recurrence rates of 0-17% [6,8,10,12,13,14,15,16,21,22,23,24]. Across all series, recurrence rate was higher in larger schwannomas. According to the literature, the most common site of recurrence is the cavernous sinus, followed by Meckel's cave [14,25]. Time taken to recur is highly variable, ranging from 1 to 9 years [6,21]. The most important factor predicting recurrence has been identified as the completeness of surgical resection [26].
In conclusion, comprehensive knowledge of the anatomical features of TSs and the selection of the most appropriate surgical approaches are essential to achieve complete resection. TSs are well to be classified with our modified classification and able to be removed effectively and safely by selecting appropriate surgical approaches.

 XML Download
XML Download