

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Xanthogranulomatous inflammation, a rare variant of chronic inflammation, is histologically characterized by lipid-laden foamy macrophages accompanied by other inflammatory cells including lymphocytes, plasma cell, neutrophil, and eosinophil (1). Although many organs such as kidney, gallbladder, gastrointestinal tract, skin, bone and genital organs involving xanthogranulomatous inflammation have been reported, xanthogranulomatous inflammation involving the pancreas is extremely rare (23). Herein, we present a case of xanthogranulomatous pancreatitis mimicking a pancreatic cancer on computed tomography (CT) and magnetic resonance imaging (MRI) in a 63-year-old man.
CASE REPORT
A 63-year-old man was transferred to our hospital for further evaluation of pancreatic cancer. He suffered from epigastric pain and dyspepsia in the past 20 days. His physical examination was unremarkable. He had no significant past medical history or family history. The patient denied any history of heavy alcohol intake and additionally, there was no history of gallstone disease, metabolic disease, smoking, or trauma. He did not have any previous attack of acute pancreatitis either. Preliminary laboratory tests were within normal limits: white blood cell count, 7.99 × 103 µL (normal range, 3.91-10.33 × 103 µL); serum amylase, 37 U/L (normal range, 25-115 U/L); and serum lipase, 10 U/L (normal range, 0-60 U/L). Tumor marker tests were also within normal limits: carcinoembryonic antigen, 1.81 ng/ml (normal range, 0-3 ng/ml); and carbohydrate antigen 19-9 (CA-19-9), 3.88 U/mL (normal range, 0-37 U/mL).
Although the patient did not bring a CT image (Fig. 1a-d) acquired at a local medical center on the first hospital visit, their radiologic report suggested pancreatic cancer with vascular invasion. For further evaluation of pancreatic cancer, the patient underwent dynamic pancreas MRI in our hospital. Dynamic pancreas MRI was performed with a 3-T system (Discovery 750; GE Healthcare, Milwaukee, WI, USA). Conventional sequences included axial and coronal heavily T2-weighted images (T2WIs), dual echo axial images, precontrast axial T1WI, contrast enhanced dynamic T1WIs (25 s, 45 s, 72 s, 10 min and 20 min) with gadoxetic acid (Primovist, Schering, Berlin, Germany) at a standard dose (0.025 mmol/kg of body weight), respiratory triggered axial T2WI with fat suppression and motion correction, axial diffusion weighted images (DWIs) (b-values = 0, 600, 800 s/mm2) and apparent diffusion coefficient maps. On pancreas parenchymal phase of MRI (Fig. 2a-d), the body and tail of the pancreas were entirely replaced by an ill-defined low signal intensity mass, showing little enhancement on dynamic phase. The mass was extended to the peripancreatic fat tissue without adjacent organ invasion. The main pancreatic duct in the tail region was dilated. On fat suppressed T2WI, the mass showed intermediate high signal intensity. The mass had subtle high signal intensity on high b-value (800 s/mm2) DWI and low signal intensity on pre-contrast T1WI. Based on these findings, our first impression was also ductal adenocarcinoma in the pancreas.
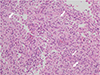
For an exact diagnosis, endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) was performed using a 22-gauge needle (EchoTip; Cook Medical Inc., Winston-Salem, NC, USA). Microscopic examination of a cell block of acquired FNA specimen showed acute and chronic inflammation with accumulation of foamy macrophages intermingled with plasma cells, neutrophils, lymphocytes, and occasional multinuclear giant cells (Fig. 3). In particular, almost all macrophages displayed eosinophilic cytoplasm with granular pattern or clear cytoplasm showing vacuolated pattern, although some macrophages were spindle shaped. No evidence of atypical cells indicating malignancy was found. These histopathology findings were consistent with findings of xanthogranulomatous inflammation. The patient underwent conservative treatment for 4 days. Since then, his condition was good and he was discharged home.
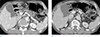
Next, we retrospectively reviewed the previous pancreas dynamic CT performed at the local medical center (LMC). When the CT image was compared to dynamic pancreas MRI, primary lesion in the body and tail of the pancreas was an expanding suspicious cystic lesion with irregular thick wall. This lesion had been changed into a mass on MRI after three weeks, strongly suggesting that the patient had a resolving stage of necrotizing pancreatitis with acute necrotic collection. Based on histologic and imaging findings, the patient was finally diagnosed as xanthogranulomatous pancreatitis. He was followed up and monitored in an outpatient clinic. Two months later, a follow-up contrast enhanced CT image revealed that the size of the low-density mass in the body and tail of the pancreas was decreased at intervals (Fig. 4a). Upstream main pancreatic duct was still dilated with hypotrophic change of pancreas parenchyma in the tail region. Six months later, a contrast enhanced CT image was performed again. The mass was markedly decreased (Fig. 4b). Since then, there have been no observable abnormalities, and he maintains an excellent quality of life.
DISCUSSION
Xanthogranulomatous pancreatitis is extremely rare. It is an idiopathic benign pathological condition of unknown etiology. Although the exact pathogenesis of xanthogranulomatous pancreatitis remains unclear, several hypotheses have been suggested. The most widely accepted pathogenesis is based on the possible theory of xanthogranulomatous pyelonephritis and cholecystitis, which obstructive condition such as stone or infection may induce xanthogranulomatous changes (4). Ueno et al. (3) have suggested that infection, necrosis and hemorrhage in the pseudocyst following acute pancreatitis might result in elevated intracystic pressure and subsequently lead to xanthogranulomatous inflammation around the wall of the pseudocyst. On the other hand, in the case of intraductal papillary mucinous neoplasm (IPMN), Kamitani et al. (4), have hypothesized that elevated intraductal pressure by mucin could result in a leak of mucin into the pancreatic parenchyma, thereby leading to xanthogranulomatous changes. In our case, when we retrospectively reviewed the initial CT image obtained at a LMC, it was notable that presumed acute necrotic collection in the body and tail of the pancreas showed expanding nature, probably elevated intracystic pressure, on initial CT image. Infection or hemorrhage in acute necrotic collection following necrotizing pancreatitis might induce xanthogranulomatous changes around the periphery of the lesion. These later stages of xanthogranulomatous changes intermingled with inflammatory cells and fibrosis mimicked solid malignant neoplasm in the pancreas.
To date, to the best of our knowledge, only 17 cases of xanthogranulomatous pancreatitis have been reported in literature (Table 1). However, the disease presentation, demographics, and risks are not specific in the previous 17 reports (1345678910). Of the 17 reported cases, xanthogranulomatous pancreatitis was more common (13 of 17) in males. The mean patient age was 57 years (range, 22 to 82 years). Majority (11 of 17) of patients presented with abdominal or epigastric pain. Some patients presented with incidental mass (2 of 17), weight loss (2 of 17), and others. (2 of 17). The locations of lesions are also not specific, including head (5 of 17), body (7 of 17), tail (4 of 17), and uncinated process (1 of 17). At the time of preoperative diagnosis, 11 patients were presumed as a true neoplastic condition, including 6 patients presumed as pancreatic cancer (158), 4 patients as IPMN (46), and one patient as solid pseudopapillary tumor (SPT) (10). The other 6 patients were suggested as having benign condition including three cases of pseudocyst (37) and three cases of chronic pancreatitis (9) through clinico-radiological correlation. Unfortunately, all patients underwent surgical resection of pancreas due to disease progression or for the exclusion of malignancy, even though 6 patients were presumed as having benign conditions before the surgery (379). Therefore, adequate diagnosis is critical in making proper decision on surgical management of pancreas. In this case, we performed EUS-FNA for the mass lesion of pancreas and demonstrated xanthogranulomatous pancreatitis. As a result, the patient underwent regular follow-up. He maintains an excellent quality of life without overtreatment such as surgical resection of pancreas.
Radiologically, differentiation from malignant tumor is essential to avoid unnecessary surgical resection. However, imaging findings and differential points have not been established yet for xanthogranulomatous pancreatitis. Given the accepted pathogenesis, xanthogranulomatous lesion might develop in the pseudocyst or during the chronological change of necrotizing pancreatitis. However, imaging findings of xanthogranulomatous pancreatitis may be different depending on the stage. In earlier stages, xanthogranulomatous change may occur in peripheral wall portion of a pseudocyst or wall-off necrosis while central cystic portion may be preserved. Ikeura et al. (10) have reported that marked infiltration of lipid-laden foamy macrophages with fibrosis is seen in the peripheral wall of the cystic mass and the central cavity contains old hemorrhage and necrotic tissue in their case. At this stage, we believe that solid and cystic or cystic mass with thick wall lesion can be misdiagnosed as SPT, IPMN and pseudocyst. However, in later stage of xanthogranulomatous pancreatitis, central necrosis or hemorrhage may be absorbed and solid lesion may be thicker or primary lesion may be replaced by marked proliferative fibrosis intermingled with lipid-laden foamy macrophages and chronic inflammatory cells. The previous cystic lesion may be disappeared at this stage. Such solid lesion might be misdiagnosed as pancreatic cancer.
In our case, the interval time between initial CT image and MRI (from suspicious cystic mass with irregular wall to the mass) was three weeks. Two months later, the solid mass was decreased in size. However, the mass was still observed with hypotrophic change of the pancreas parenchyma. After six months, the size of solid mass was markedly decreased. Given that all reported 17 cases underwent surgical resection, our case showing serial image changes of proven xanthogranulomatous pancreatitis by EUS- FNA will be clinically meaningful.
In conclusion, although xanthogranulomatous pancreatitis is unfamiliar to many radiologists without published reports focusing on its radiologic findings, it should be noted that xanthogranulomatous pancreatitis can be clinically or radiologically misinterpreted as malignant neoplasms. Based on our case, preoperative EUS-FNA may prevent misdiagnosis and overtreatment of patients with xanthogranulomatous pancreatitis.



 XML Download
XML Download