

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Traumatic spinal subarachnoid hemorrhage (SSAH) and spinal subdural hemorrhage (SSDH) are very rare. Most cases occur as a complication of spinal procedures such as spinal anesthesia and are often associated with blood coagulation abnormalities, such as anticoagulation therapy or thrombocytopenia.2) Traumatic SSAH or SSDH can occur at the site of the spinal injury, but several cases of traumatic SSAH or SSDH that was supposed to be migration of intracranial traumatic subarachnoid hemorrhage (SAH) or subdural hemorrhage (SDH) without direct spinal injuries were reported.12368) Of them, reports of traumatic SSAH migrated from intracranial traumatic SAH are extremely rare.2)
Here, we report a case of SSAH migrated from traumatic intracranial SAH in a patient without direct spinal injury.
Case Report
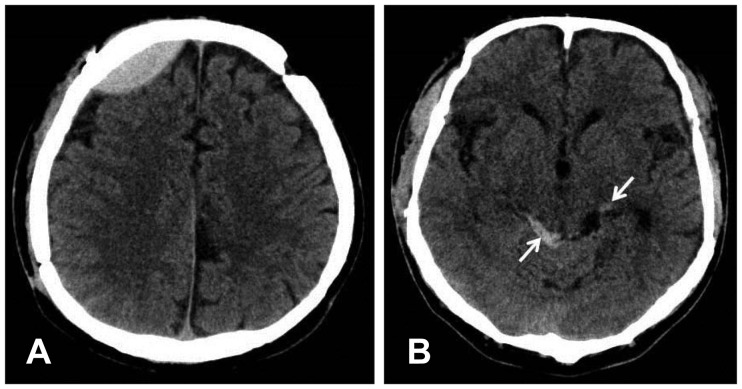
A-59-year-old male presented with headache after traumatic brain injury (TBI). He had hit his head on the corner of a desk and had lost his consciousness a few seconds an hour before. He did not complain of pain in other parts of his body except for his headache. On neurological examination, Glasgow Coma Scale was 15 and no motor or sensory changes were found. He had had a history of TBI and had undergone bilateral craniotomy and removal of epidural hematoma (EDH) 5 years prior. He had no previous medical problems and took no medication. A brain computed tomography (CT) scan revealed EDH in the right frontal lobe and traumatic SAH in the ambient cistern (Figure 1). Due to his stable clinical condition, no immediate surgical treatment was planned. Instead, he was admitted for close monitoring of his neurological status.
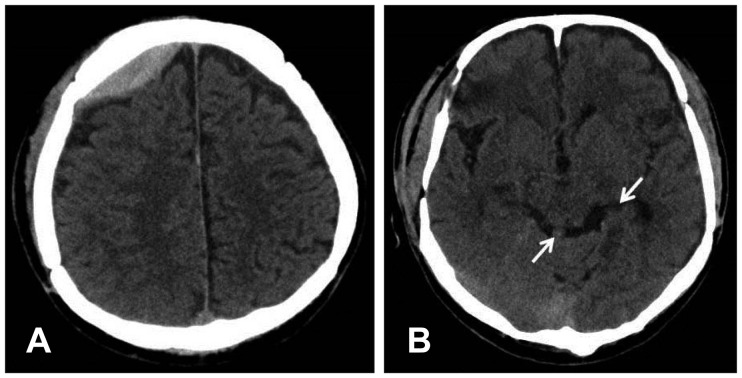
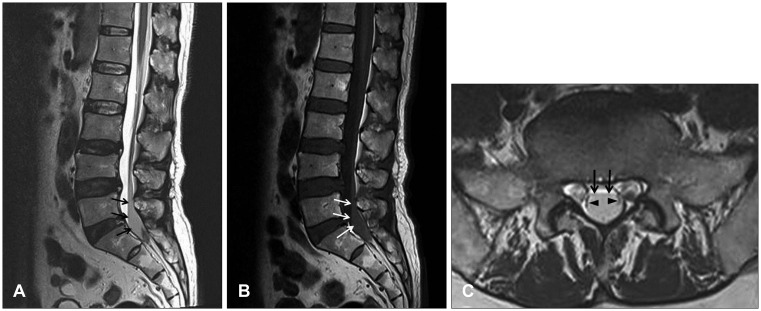
Two days after TBI, he complained of pain and numbness in the bilateral buttock and posterior thigh. A lumbar spine plain radiograph showed no fracture or dislocation. His pain and numbness progressively worsened. On the next day, he could not sit or stand due to severe pain and numbness. Perianal numbness and voiding difficulty began. A Foley catheter was placed and 500 cc of urine was drained. On neurological examination, motor weakness in the lower extremities was not evident. A follow-up brain CT scan showed a slight decrease in the thickness of EDH, and SAH was much resolved (Figure 2). Lumbar spine magnetic resonance imaging (MRI) revealed a fusiform lesion within the dorsal part of the spinal canal at the L5 and S1 level. The cauda equina was compressed and displaced laterally. The lesion had low signal intensity in the T2-weighted image (WI) and iso-signal intensity in the T1-WI, suggestive of acute hemorrhage (Figure 3). Contrast enhancement images showed no abnormally enhanced lesion.
A diagnosis of cauda equina syndrome due to intraspinal hemorrhage was made and emergent operation was performed. After a partial laminectomy of S1, the dural sac was exposed and no EDH was found. The dural sac was tense on palpation. When opening the dura, SDH was not found. On incision of the arachnoid membrane, dark reddish fluid gushed out with high pressure. No blood clot and no definite bleeding point were found. The pain and numbness disappeared immediately after the surgery. He had gradual improvement in his voiding function. At his 1-year-follow-up, he had no subjective discomfort in his voiding function.
Discussion
Traumatic intracranial hemorrhage can cause intraspinal hemorrhage in patients without any direct injury to the spine as in the present case.12368) SSDH can occur in patients with traumatic intracranial SDH.168) Because of the anatomic continuity between the intracranial and spinal subdural spaces, redistribution or migration of the intracranial SDH to the spinal subdural space can occur.16) If an arachnoid tear exists, this might facilitate spontaneous resolution and migration of intracranial SDH by a dilutional and "water hammer" like effect of cerebrospinal fluid (CSF) that leaks from the subarachnoid space to the subdural space through the arachnoid tear.8) Furthermore, raised intracranial pressure due to intracranial SDH can push the hematoma directly into the skull base and spinal canal through the subdural space.4)
Although not a traumatic etiology, cases of SSDH occurring in patients with intracranial SAH have been reported.47) SAH under high pressure can tear the intact arachnoid membrane, extravasate the SAH into the subdural space, and cause intracranial SDH or SSDH.4) If an arachnoid tear already exists, intracranial SAH might migrate into the subdural space through the arachnoid tear, and this can develop into intracranial SDH or SSDH.4)
Cerebral contusion can also cause SSAH. There was a case report of SSAH in a patient with cerebral contusion in the temporal lobe.3) One day after admission, the patient complained of neck pain, followed by severe right hemiparesis, dysphagia, and hoarseness. CT scan revealed progression of the contusion and intraspinal hemorrhage extending to the C3 level with the brain stem and the spinal cord displaced contralaterally. SSAH was detected intraoperatively and the authors suggested that the progression of the initial temporal lobe contusion made the blood spread into the adjacent subarachnoid spaces. This intracranial SAH might have migrated to the upper cervical level. The cisterns of the posterior cranial fossa include the prepontine, interpeduncular, cerebellopontine, premedullary, cerebellomedullary, quadrigeminal, superior cerebellar cisterns, and the cisterna magna. The ambient cistern communicates with the interpeduncular cistern. The anterior and posterior spinal cisterns communicate with cisterns of the posterior cranial fossa through the foramen magnum. Therefore, intracranial SAH can migrate to the spinal subarachnoid space.3) This migration occurs with higher probability in patients with a large amount of SAH or after early ambulation of the patient.3)
SSAH can occur in patient with traumatic intracranial SAH as in the present case. Chen et al.2) reported a case of SSAH in a patient with traumatic SAH within the left sylvian cistern. After admission, the patient began complaining of numbness in the left posterior thigh and a heavy sensation in the legs. Lumbar spine MRI 9 days after the initial trauma showed a fusiform lesion located at the L5 and S1 level. During surgery, an old blood clot was removed after opening the arachnoid membrane. The authors hypothesized that migration of blood could have occurred from the intracranial subarachnoid space to the subarachnoid space at the most caudal part of the spinal canal.2) In the present case, the patient complained of no low back or buttock pain immediately after the trauma. The patient presented pain and numbness with delayed onset and symptoms worsened rapidly. Intracranial SAH was much resolved and no traumatic lesion in the lumbosacral spine was found in the radiologic evaluation when the patient began complaining of pain. Therefore, we hypothesize that the SSAH might have been related to progressive migration of intracranial SAH in the ambient cistern to the most dependent area of the lumbosacral subarachnoid space through the above mentioned pathways. Contrary to Chen et al.'s2) report, we found uncoagulated dark red blood rather than an old blood clot intraoperatively. In our opinion, this might have resulted from the different timing of the operation. In the present case, operation was performed 3 days after the initial trauma, as compared to surgery being performed 9 or more days after the trauma in Chen et al.'s2) report. SSAH rarely forms a hematoma owing to the continuous diluting or "washing" effect of the CSF.25) Interestingly, migration of the blood can occur in reverse direction, that is, from the spine to the brain.910) Although not a traumatic etiology, there were reports in which intracranial SAH or SDH was found later during the workup for SSDH or SSAH.910) In the present case, although the onset of symptoms was delayed, the deterioration of symptoms was rapid, as in other reports.138) Therefore, a suspicion of intraspinal hemorrhage and prompt radiologic workup should be performed in patients with traumatic intracranial SAH or SDH who present with delayed pain or neurologic deficit.
Conclusion
We suggest that delayed intraspinal hemorrhage may occur in patients with TBI. In particular, patients who have traumatic intracranial SAH or SDH and who present with delayed pain or neurological deficits should be evaluated for SSAH or SSDH promptly, even when the patients had no history of direct spinal injury and had no apparent symptoms related to the spinal injury in the initial period of trauma.
 XML Download
XML Download