

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hashimoto's encephalopathy (HE) is a rare neurological disorder with a heterogeneous group of neurological symptoms.1 Sporadic Creutzfeldt-Jakob disease (CJD) is the most common human prion disease and usually manifests as a rapidly progressive dementia, with ataxia and myoclonus leading to death in less than 1 year.2 CJD shares common clinical features with HE, and dementia, myoclonus, extrapyramidal signs, ataxia, psychotic phenomena and personality changes characterize both diseases.3 The presence of 14-3-3 protein in the cerebrospinal fluid (CSF) is a useful marker for in vivo diagnosis of CJD. 14-3-3 protein is a relatively sensitive and specific marker of CJD and is not commonly detected in HE. We report the case of a patient with HE with unusual features, including positive 14-3-3 protein in the CSF, and an atypical course mimicking that of CJD.
CASE REPORT
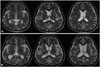
A 64-year-old male visited the hospital with progressively deteriorating cognitive function and abnormal behavior for 3 days. There were no specific findings in disease, drug, social, or family history. The patient complained of systemic fatigue and showed a dull demeanor and more-sluggish activity than usual. The patient was lucid, but showed impaired orientation regarding time, place, and person. He gave inappropriate answers to most questions and was able to perform tasks only after several repetitions of simple instructions. There was no apparent decrease in muscle power, and all sensory functions and the deep tendon reflex were normal, with no pathological reflexes. The cerebellar function test was normal, but frontal releasing signs, such as the glabellar reflex and palmomental reflex, were positive, and ideomotor apraxia of both hands was observed. The Korean Mini-Mental Status Examination (MMSE) score was decreased to 16 points, and all domains of the Seoul Neuropsychological Screening Battery showed deterioration. The results of complete blood count, blood chemistry, syphilis reaction test, and vitamin B12 test were within normal limits, and levels of viral markers and autoimmune antibodies (RF, ANA, ANCA, C3, C4, anti-mitochondrial Ab, antidsDNA Ab, anti-Ro Ab, anti-La Ab, etc.) were within normal limits or negative. Paraneoplastic syndrome selection tests, including serum anti-Hu, anti-Yo, and anti-Ri, were normal. In the thyroid function test, TSH was 1.00 µIU/m and free T4 was 1.04 ng/dL, both normal values, but T3 was decreased at 55.66 ng/dL. Anti-thyroid microsomal Ab and anti-thyroglobulin Ab levels were increased at 0.33 U/mL and 0.70 U/mL, respectively. The CSF test showed a normal intracranial pressure of 11 cm H2O, and a normal red blood cell (RBC) count of 2/µL, but the white blood cell (WBC) count was increased to 54/µL (85% lymphocytes), and the protein level was increased at 64.5 mg/dL. Antibodies for anti-Hu, Yo, Ri, MA2, CV2/CRMP5, amphiphysin, recoverin, SOX1, titin, NMSAR, AMPA1, AMPA2, LGI1, CASPR2, and GABA-B in the CSF were negative, and 14-3-3 protein was weakly positive in the Western blot. High signal intensities were observed in the bilateral basal ganglia, the thalamus, and multifocal areas in the cerebral hemispheres in T2-weighted image (T2WI) and fluid-attenuated inversion recovery (FLAIR) image on brain magnetic resonance imagining (MRI) (Fig. 1A). The brain electroencephalogram (EEG) showed mostly slow waves with no epileptiform spikes (Fig. 2A). After admission, the patient showed progressive worsening of abnormal behavior, and although viral antibodies were not found in the CSF, because the patient showed an increase in WBC count with lymphocyte predominance, he was treated with acyclovir 1980 mg/day intravenous due to a diagnosis of idiopathic viral encephalitis, but showed no significant clinical improvement. Although TSH was normal, T3 was slightly decreased and anti-thyroid microsomal Ab and anti-thyroglobulin Ab levels were increased in the TFT. Under the suspicion of HE caused by Hashimoto's thyroiditis, which is the most common cause of asymptomatic hypothyroidism, the patient was given highdose steroids (methylprednisolone 1000 mg/day) for 5 days and was maintained with oral prednisolone. He showed a clear improvement in cognitive function after initiation of treatment. The patient received a score of 22 in the MMSE performed 10 days after initiating steroid treatment, which is an improvement compared to the previous score, and particular improvement in the areas of orientation and memory retrieval was evident. The patient was discharged from the hospital after stopping oral steroid treatment, but the disorientation and abnormal behavior symptoms slowly began to recur after 2 months, and he was readmitted. The CSF test results showed an intracranial pressure of 14 cm H2O and RBC count of 2/µL, which is normal, but the WBC count was 48/µL (72% lymphocytes) and the protein level was increased at 54 mg/dL, and 14-3-3 protein was positive in Western blot. TSH was 1.23 µIU/m and free T4 was normal at 1.08 ng/dL, but T3 was decreased at 38.91 ng/dL, and although the anti-thyroid microsomal Ab level was normal at 0.18 U/mL, the anti-thyroglobulin Ab level was increased to 0.47 U/mL. With the symptom recurring, high-dose steroids (methylprednisolone 1000 mg/day) were given intravenously for 5 days. Symptoms improved accordingly, and the patient was discharged. However, 2 weeks later the patient revisited the hospital due to generalized seizures, and the neurological examination showed left upper-limb weakness, bilateral upper limb myoclonus, opsoclonus, visual hallucinations and optic ataxia. He also showed a tendency to lean to both sides due to trunk impairment. The patient was unable to perform simple tasks due to severe cognitive impairment and apraxia and it was difficult to understand what the patient was saying due to dysarthria. He also could not form proper sentences. The CSF test showed an intracranial pressure of 12 cm H2O, a WBC count of 3/µL, and a protein concentration of 26 mg/dL, which is normal. 14-3-3 protein was positive in the Western blot, but the tau protein level decreased from 2704.3 pg/mL to 205.7 pg/mL, which is a finding inconsistent with typical CJD. Bilateral frontoparietal cortical atrophy was observed in the brain MRI, and the high signal intensity in the bilateral cerebral cortex, subcortical white matter, right thalamus, and midbrain in the FLAIR and T2WI was shown (Fig. 1B). Angiography performed to differentiate primary central nervous system (CNS) angiitis showed no significant stenosis or occlusion of the cranial arteries. Whole-body positron emission tomography (PET) was performed to rule out paraneoplastic syndrome, but no abnormalities were observed. The brain EEG showed periodic lateralized epileptiform discharges across the entire right cranial hemisphere (Fig. 2B). Lorazepam and phenytoin were injected intravenously to control the seizures and were maintained orally thereafter, but 7 days later the patient showed status epilepticus, which is a state in which multiple seizures occur with no recovery of consciousness, and was given levetiracetam intravenously, upon which no further seizures occurred. Slowly progressing dementia, myoclonal seizures, generalized seizures, optic ataxia, cerebellar symptoms, visual hallucinations, and dysarthria suggested a diagnosis of recurrent HE, and high-dose steroid (methylprednisolone 1000 mg/day) were readministered for 5 days, but symptoms did not improve. Disorientation, memory loss, and optic ataxia are still apparent at the time of writing, after 5 months.
DISCUSSION
Our case of HE showed progressive cognitive dysfunction with relapsing and remitting course and positive 14-3-3 protein in CSF. The clinical manifestations of HE may mirror that of CJD, and the two diseases can be confused.4 HE can be distinguished from CJD based on several features. First, a positive response to steroid treatment is an important identifying characteristic of HE.5 Another distinguishing point is the presence of seizures, which is common in HE but rare in CJD.6 Moreover, the presence of periodic spike wave discharges on EEG2 and characteristic MRI findings of T2/FLAIR and diffusion weighted imaging (DWI) pattern in the basal ganglia7 are also helpful in distinguishing the two conditions. Our patient showed a definite response to steroid pulse therapy, frequent seizure attacks, absence of periodic spike wave discharges on EEG and nonspecific diffuse white matter changes on MRI. However, 14-3-3 protein was positive in CSF. Although the presence of 14-3-3 protein is commonly associated with CJD, there are two reports of HE cases with positive 14-3-3 protein.48 Elevated 14-3-3 protein levels have been also reported in patients with stroke, CNS infections, intracranial metastasis and metabolic encephalopathy.9 In view of these findings, 14-3-3 protein is considered to be a general marker of neuronal destruction and not a specific tool for the identification of CJD.
Clinical subtypes of HE are proposed as a vasculitic type with relapsing and remitting course and another subtype with a progressive course of significant decline in cognitive function. Our patient showed a relapsing and remitting course of cognitive function and an excellent initial response to steroid treatment. Over time, his cognitive dysfunction worsened, and new psychiatric symptoms developed. Furthermore, opsoclonus-myoclonus syndrome, which is a common feature of paraneoplastic limbic encephalitis (PLE), was observed and was not improved by steroid pulse therapy. MRI findings did not reveal temporal lobe abnormalities and no primary malignancy was detected by whole-body PET. The clinical manifestations of HE are variable and its diagnosis is difficult due to the absence of a specific phenotype pattern. A decreased response to steroid or opsoclonus-myoclonus resembling PLE is rarely reported in HE. The differential diagnosis is broad and includes CNS infection, autoimmune-related encephalopathy, neurodegenerative disease and PLE. Likewise, other possible causes should be ruled out before making a diagnosis of HE.
In conclusion, we recommend that patients with clinical features of CJD and antithyroid antibodies should be considered for empirical steroid treatment for HE, despite being positive for 14-3-3 protein.

 XML Download
XML Download